If you have been living with ringing, buzzing, humming, or hissing in your ears and wondering what is actually causing it — you are asking exactly the right question.
Most people assume tinnitus is an ear problem. Something went wrong with the ear, the ear is making noise, fix the ear and the noise stops.
If only it were that simple.
The reality of what causes tinnitus is considerably more interesting — and understanding it properly changes everything about how you approach managing the condition. So let us start at the beginning.
What Is Tinnitus, Exactly?
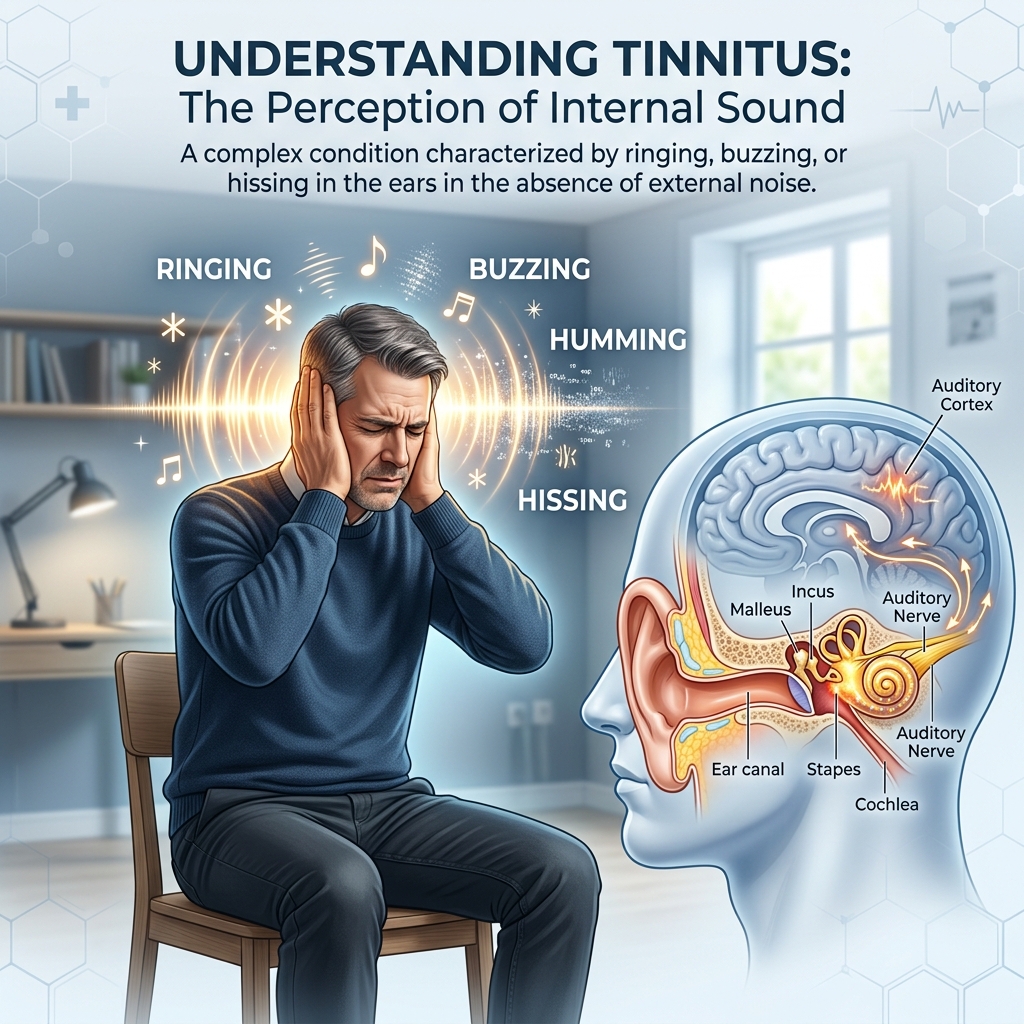
Tinnitus — pronounced either “tin-NITE-us” or “TIN-uh-tus” — is the perception of sound that has no external source. The ringing, buzzing, humming, hissing, clicking, or roaring you hear is not coming from your environment. Nobody else in the room can hear it. It is being generated internally.
According to the National Institutes of Health, tinnitus affects between 10 and 25 percent of adults — including more than 50 million people in the United States alone. It is more common than most people realise, and yet it remains one of the most misunderstood conditions in audiology.
The most important thing to understand about tinnitus is this: it is a symptom, not a disease. It is your body’s way of signalling that something in the auditory system — or the systems connected to it — is not functioning normally.
What that something is varies enormously from person to person. Which is exactly why tinnitus can feel so difficult to address.
Read Also: Is Tinnitus Permanent? The Honest Answer Nobody Tells You
Where Does the Sound Actually Come From?
Before we get into the specific causes, it is worth understanding the mechanism — because it explains a lot about why certain causes trigger tinnitus while others do not.
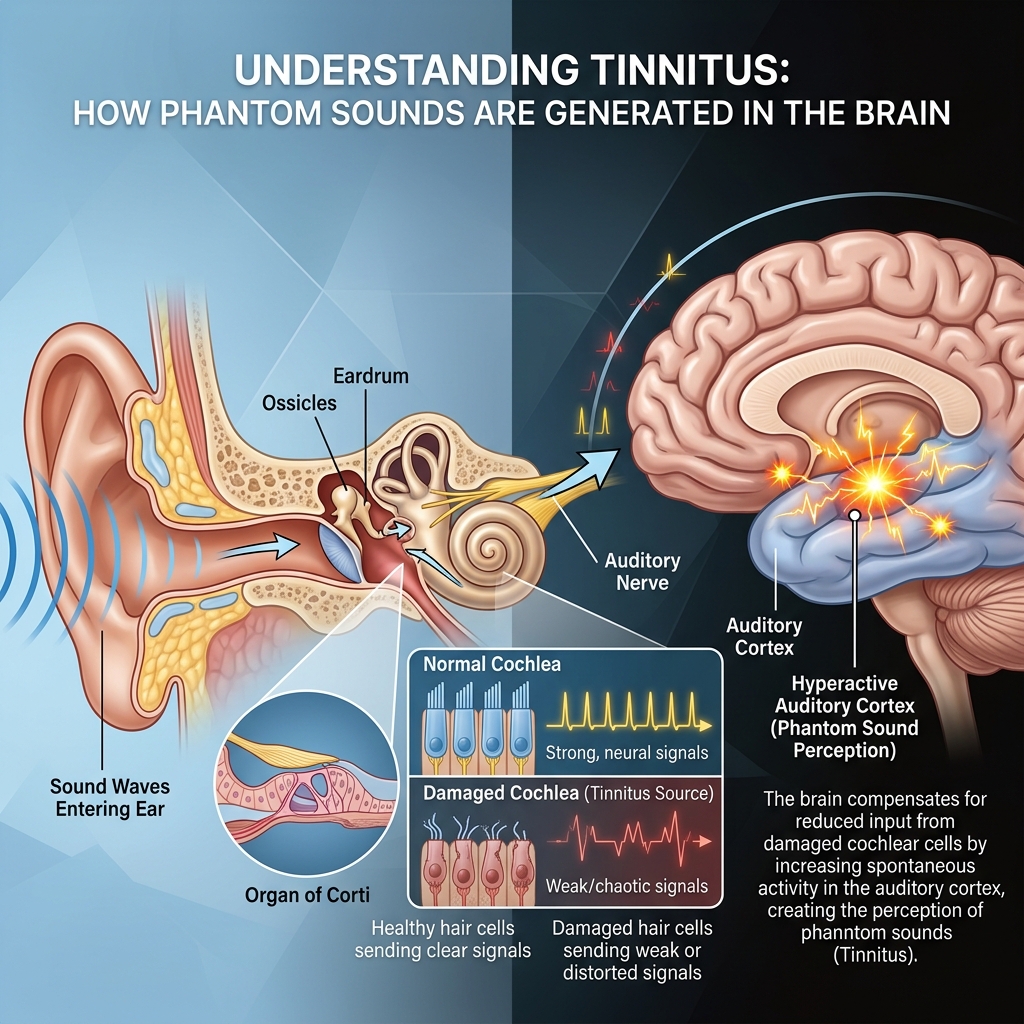
Your inner ear contains thousands of microscopic hair cells inside the cochlea — the fluid-filled, snail-shaped structure that converts sound waves into electrical signals. These signals travel along the auditory nerve to the brain, where they are interpreted as sound.
When these hair cells are healthy and functioning normally, the process works seamlessly. When they become damaged, bent, or destroyed — through any of the causes we are about to discuss — the signals they send to the brain change.
Here is the critical part: your brain does not simply go quiet in response to reduced or distorted input. Instead it compensates. The auditory cortex — the brain region that processes sound — increases its own activity to make up for the reduced input from the damaged cochlea. In doing so, it generates its own phantom sounds.
Research from the National Institutes of Health confirms that tinnitus is largely a brain phenomenon — not an ear phenomenon. The sound you hear is being created by your auditory cortex, even though it feels like it is coming from your ear.
This distinction matters enormously for understanding what causes tinnitus and what can actually help manage it.
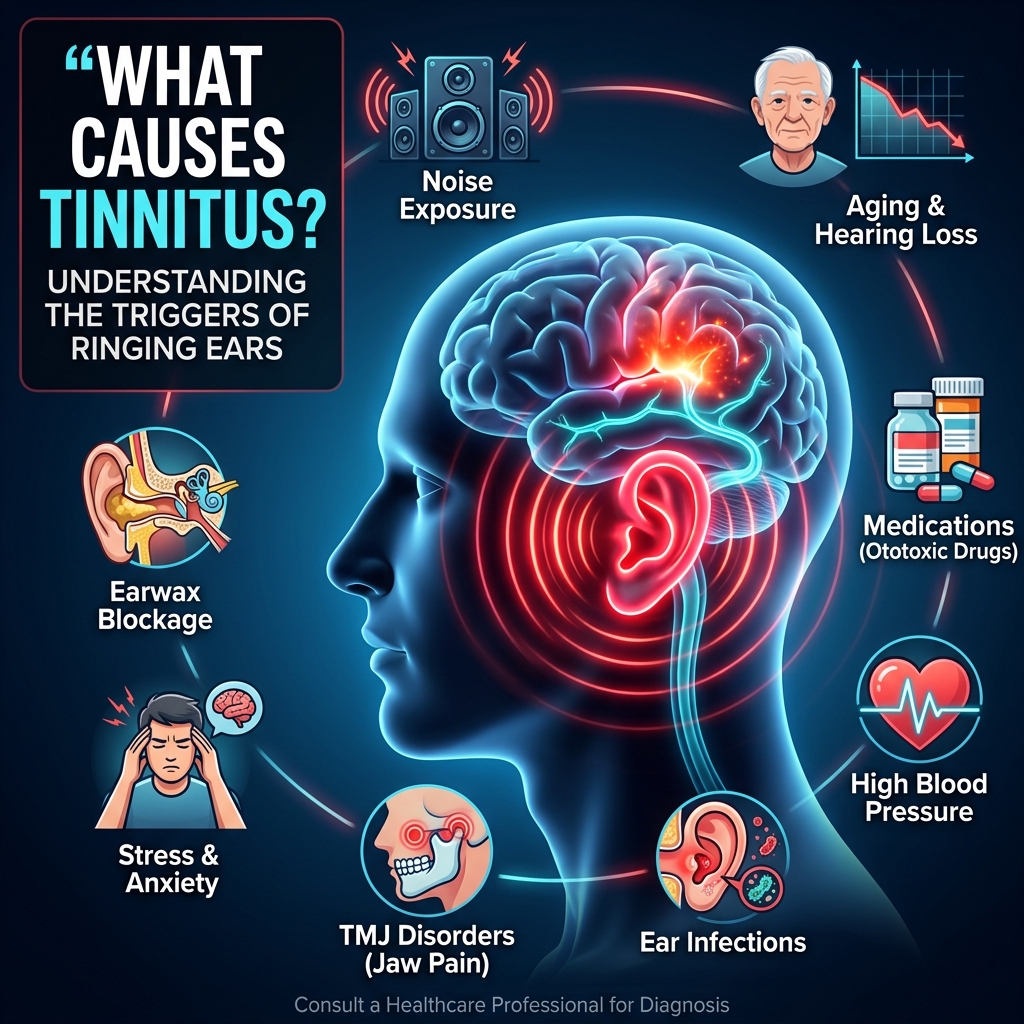
The Most Common Causes of Tinnitus
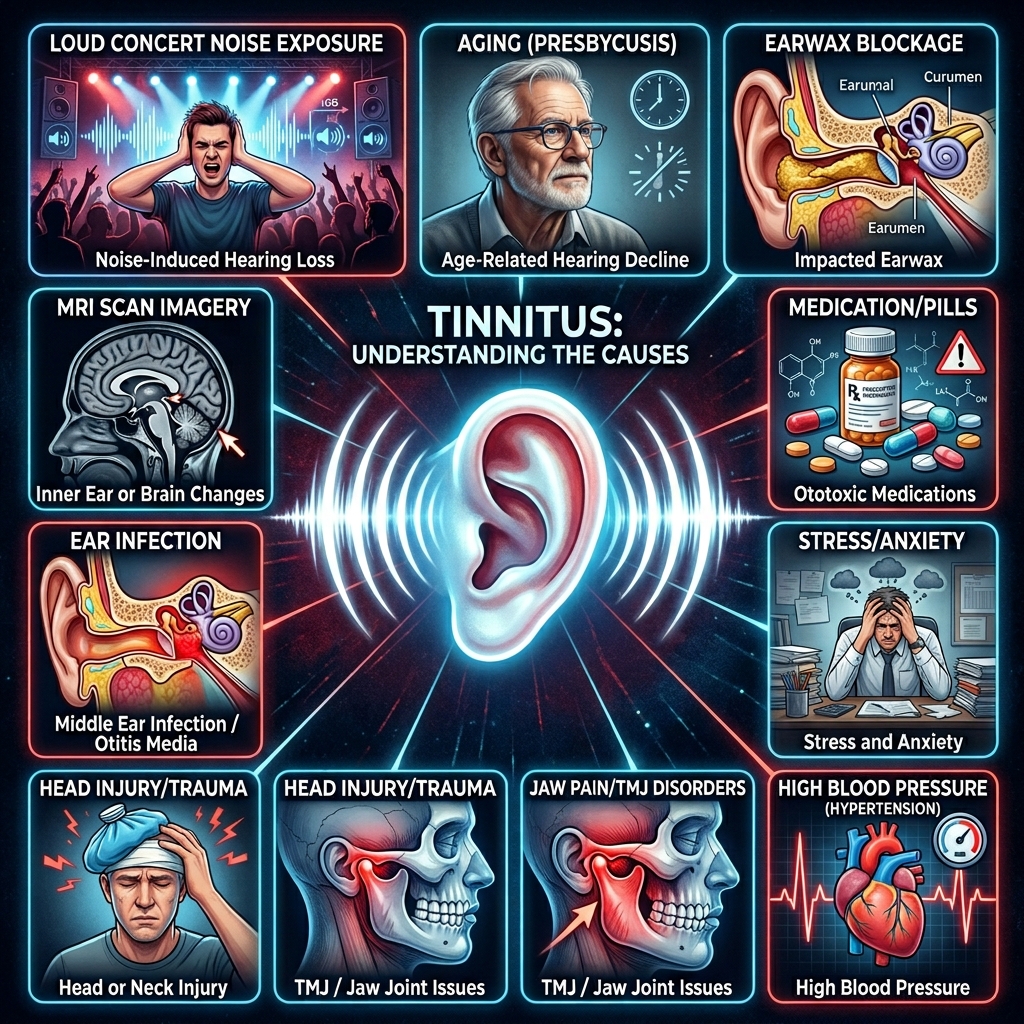
1. Age-Related Hearing Loss (Presbycusis)
This is the single most common cause of tinnitus worldwide — and the most inevitable one for most people if they live long enough.
As we age, cochlear hair cells gradually deteriorate. This is a natural process that begins in early adulthood and accelerates after fifty. As more hair cells are lost or damaged, the signals reaching the auditory cortex become weaker and less complete.
The brain compensates by turning up its own internal gain — essentially amplifying its processing to make up for the reduced input. This increased neural activity manifests as phantom sounds: ringing, buzzing, humming.
About one in three adults over sixty-five experiences tinnitus as a result of age-related hearing loss. It is the reason tinnitus becomes more common with age — not because aging itself causes tinnitus, but because aging causes the hearing loss that triggers the brain’s compensatory response.
The difficult truth about this cause is that cochlear hair cells in humans do not regenerate. Once lost, they are gone. This is why age-related tinnitus tends to be chronic rather than temporary. Management rather than cure becomes the realistic goal.
2. Noise-Induced Hearing Loss
Loud noise is the most preventable cause of tinnitus — and also one of the most common.
Exposure to sounds above 85 decibels — the level of heavy city traffic, a lawn mower, or a loud restaurant — can begin damaging cochlear hair cells over time. Exposure to sounds above 120 decibels — a rock concert, a chainsaw at close range, a gunshot — can cause immediate and permanent damage.
The hair cells most vulnerable to noise damage are those that respond to high-frequency sounds — which is why noise-induced tinnitus often presents as a high-pitched ringing rather than a low hum.
Tinnitus is the number one service-related disability among military veterans — a direct consequence of exposure to firearms, machinery, and explosive blasts without adequate hearing protection.
What makes noise-induced hearing loss particularly insidious as a cause of tinnitus is its cumulative nature. A single concert might produce temporary ringing that resolves within a day. But years of concerts, earbuds at high volume, noisy workplaces, and recreational noise exposure accumulate into permanent cochlear damage that eventually produces chronic tinnitus.
The damage is happening long before the tinnitus appears.
3. Earwax Buildup and Ear Canal Blockage
This is one of the most easily overlooked and most easily resolved causes of tinnitus — which makes it particularly worth checking early in any tinnitus investigation.
Earwax is a normal and healthy secretion that protects the ear canal from bacteria, debris, and foreign particles. Problems occur when it accumulates to the point where it presses against the eardrum, altering the pressure in the ear and disrupting normal sound transmission.
The resulting tinnitus is often accompanied by muffled hearing and a feeling of fullness or blockage in the affected ear. It can appear suddenly if a piece of compacted wax shifts position, or gradually as wax builds up over time.
The good news: once the blockage is professionally cleared — through ear drops, irrigation, or microsuction performed by a healthcare provider — the tinnitus typically resolves completely and quickly.
Cotton buds are not the answer. They compact wax deeper into the canal and increase the risk of eardrum perforation. If earwax blockage is suspected, see a pharmacist or doctor.
4. Ear and Sinus Infections
Middle ear infections — otitis media — cause inflammation and fluid buildup behind the eardrum. This fluid changes the pressure in the middle ear, disrupts the normal vibration of the eardrum and ossicles (the tiny bones that transmit sound), and can produce tinnitus in the affected ear.
Sinus infections can have a similar effect by creating pressure changes that radiate into the ear through the Eustachian tube.
Infection-related tinnitus is almost always temporary — it resolves once the infection is treated and the fluid clears. If tinnitus appeared around the same time as a cold, flu, or feeling of ear fullness and pain, infection is a strong candidate.
This is also why the Mayo Clinic recommends seeing a doctor if tinnitus develops after an upper respiratory infection and does not improve within a week — it suggests the infection has not fully cleared.
5. Medications
A surprisingly wide range of medications can cause or worsen tinnitus as a side effect. This type of drug-induced tinnitus is called ototoxicity — meaning the medication is toxic to the auditory system.
The most commonly implicated medications include:
Non-steroidal anti-inflammatory drugs (NSAIDs): Aspirin, ibuprofen, and naproxen — particularly at high doses — are well-established causes of tinnitus. The effect is often dose-dependent and reversible when the medication is stopped or reduced.
Certain antibiotics: Aminoglycoside antibiotics — including gentamicin and streptomycin — are known to cause permanent cochlear damage at high doses. They are used only when no safer alternative exists.
Cancer chemotherapy drugs: Platinum-based drugs like cisplatin are strongly ototoxic and produce tinnitus and hearing loss in a significant proportion of patients.
Diuretics (water pills): Loop diuretics like furosemide can cause temporary or permanent tinnitus, particularly at high intravenous doses.
Antimalarial medications: Quinine and related compounds have been known to cause tinnitus since the nineteenth century.
Some antidepressants: Particularly at higher doses, certain antidepressants can produce tinnitus as a side effect.
If tinnitus appeared shortly after starting a new medication, it is worth raising with your prescribing doctor. In many cases, adjusting the dose or switching to an alternative medication resolves the tinnitus. Never stop prescription medication without medical guidance.
6. High Blood Pressure and Vascular Conditions
Tinnitus and cardiovascular health are more closely connected than most people realise.
High blood pressure forces blood through the vessels near the inner ear with increased force and turbulence. When this turbulent blood flow is close enough to the cochlea or auditory nerve to be detected by the auditory system, the result is pulsatile tinnitus — a rhythmic whooshing, pulsing, or beating sound that occurs in time with the heartbeat.
Pulsatile tinnitus is distinct from the more common constant ringing type and is more likely to have a cardiovascular cause. It warrants specific medical investigation — including imaging tests — to rule out vascular abnormalities.
Beyond blood pressure, other vascular causes of tinnitus include:
Atherosclerosis: Narrowing and stiffening of blood vessel walls creates turbulent blood flow that can produce audible sounds near the ear.
Arteriovenous malformations: Abnormal connections between arteries and veins near the ear can produce pulsatile tinnitus.
Carotid artery disease: Narrowing of the carotid arteries in the neck can produce sounds audible to the ear.
Managing blood pressure through diet, exercise, and medication where appropriate is one of the most impactful things people with cardiovascular tinnitus can do to reduce symptom severity.
7. Head and Neck Injuries
Physical trauma to the head, neck, or jaw can damage the inner ear, auditory nerve, or the brain regions responsible for auditory processing — resulting in tinnitus that often presents in one ear only on the side of the injury.
Even relatively minor injuries can cause tinnitus. Whiplash from a car accident, a blow to the side of the head, dental procedures that strain the temporomandibular joint, or even a particularly vigorous sports collision can all trigger or worsen tinnitus through their effect on the surrounding structures.
A specific subset worth mentioning is somatosensory tinnitus — where the tinnitus is modulated by movements of the head, neck, or jaw. If turning your head, pressing on your neck muscles, or clenching your jaw changes the pitch or volume of your tinnitus — somatosensory involvement is likely and physiotherapy or dental treatment may help.
8. TMJ Disorders
The temporomandibular joint — the hinge connecting the lower jaw to the skull — sits directly adjacent to the ear canal on both sides. When this joint becomes inflamed, misaligned, or damaged through clenching, grinding, or injury, its proximity to the ear means the effects are directly felt in the auditory system.
TMJ-related tinnitus is often one-sided, frequently accompanied by jaw pain or clicking, and characteristically changes or fluctuates with jaw movements.
People who grind their teeth at night — a condition called bruxism — are particularly susceptible to TMJ-related tinnitus. The nightly strain on the joint creates chronic inflammation that progressively affects the surrounding ear structures.
A dentist or maxillofacial specialist can assess TMJ function and recommend appropriate treatment — which often includes a custom night guard, physiotherapy, or specific jaw exercises.
9. Ménière’s Disease
Ménière’s disease is an inner ear disorder characterised by episodes of severe vertigo, fluctuating hearing loss, and tinnitus — typically in one ear only.
The underlying mechanism involves abnormal fluid pressure in the endolymph — the fluid that fills the inner ear chambers. When this pressure builds beyond a threshold, it triggers an episode: sudden severe dizziness that can last minutes to hours, accompanied by intensified tinnitus and muffled hearing in the affected ear.
Between episodes, tinnitus may persist at a lower intensity. Over time, episodes can cause progressive and permanent hearing loss in the affected ear.
Ménière’s disease is diagnosed by an ENT specialist based on the pattern of symptoms. Management includes dietary changes (particularly sodium restriction), medications to control dizziness and fluid balance, and in severe cases, surgical intervention.
10. Stress, Anxiety and Mental Health
The relationship between tinnitus and psychological state is bidirectional and profound — and it is one of the most underappreciated aspects of what causes tinnitus to flare up or worsen.
Chronic stress elevates cortisol levels, increases systemic inflammation, disrupts sleep, and heightens the sensitivity of the nervous system to all stimuli — including the auditory system. For people with existing tinnitus, high stress reliably makes the ringing louder, more intrusive, and harder to ignore.
For some people, acute psychological stress can appear to trigger tinnitus that was not previously noticeable — though in most cases it is more accurate to say that stress amplified existing low-level tinnitus to the point where it became impossible to ignore.
The tinnitus and stress cycle is clinically documented and genuinely vicious: stress worsens tinnitus, worsening tinnitus increases anxiety, increased anxiety worsens sleep, poor sleep increases cortisol, higher cortisol worsens tinnitus further.
Breaking this cycle is one of the most important — and most difficult — aspects of tinnitus management. Cognitive Behavioural Therapy has the strongest evidence base for addressing this psychological dimension of tinnitus.
11. Acoustic Neuroma
An acoustic neuroma — more accurately called a vestibular schwannoma — is a benign tumour that develops on the vestibular nerve connecting the inner ear to the brain. As it grows, it can compress the adjacent auditory nerve, causing tinnitus and progressive hearing loss — almost always in one ear only.
Acoustic neuromas are rare and they grow very slowly. They are non-cancerous and very treatable when detected. But they are the specific reason that persistent one-sided tinnitus — particularly when accompanied by any degree of hearing change — should be properly evaluated with imaging rather than self-monitored indefinitely at home.
An MRI scan can rule out an acoustic neuroma quickly and definitively. If you have one-sided tinnitus with no obvious cause and your doctor has not yet recommended imaging, it is worth asking specifically about this.
12. Other Medical Conditions
A number of other systemic conditions are associated with tinnitus — not as direct causes, but as contributors that affect the auditory system through broader physiological effects:
Diabetes: Affects blood vessel health throughout the body, including the tiny vessels supplying the cochlea. Poorly controlled diabetes is associated with higher rates of tinnitus and hearing loss.
Thyroid disorders: Both hypothyroidism and hyperthyroidism have been linked to tinnitus — through effects on circulation, fluid balance, and neural function.
Anaemia: Reduced red blood cell count means reduced oxygen delivery to the cochlea. The resulting compensatory increase in blood flow can produce sounds audible to the auditory system.
Autoimmune conditions: Lupus, rheumatoid arthritis, and multiple sclerosis have all been associated with tinnitus through their inflammatory effects on the auditory system.
If you have a known chronic health condition and are experiencing tinnitus, mention the connection to your managing physician — better control of the underlying condition often improves tinnitus.
Why Identifying Your Cause Matters
Reading through this list, you may have noticed that the causes of tinnitus range enormously — from something as simple as earwax to something as complex as neural circuit reorganisation in the auditory cortex.
This is why tinnitus is so frequently mismanaged. When the cause is not properly identified, treatment is essentially guesswork. And because no single treatment works for all types of tinnitus, the wrong approach wastes time and creates frustration.
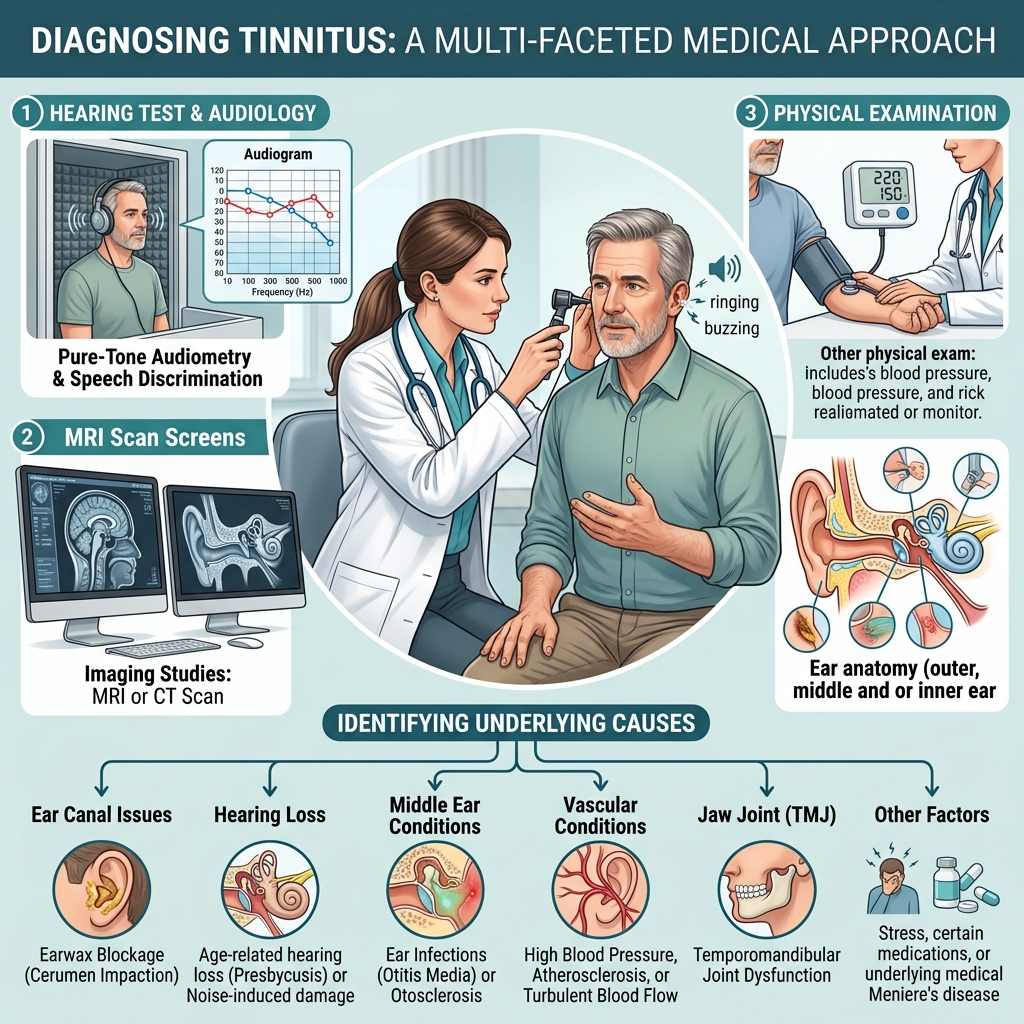
The diagnostic process typically involves:
A thorough medical history — when did the tinnitus start, what does it sound like, is it constant or intermittent, does anything make it better or worse, what medications are you taking.
A physical examination — checking the ear canal for wax or obstruction, examining the eardrum, checking blood pressure.
Audiological testing — a hearing test to assess whether hearing loss is present and at which frequencies.
Imaging — an MRI or CT scan if pulsatile tinnitus, one-sided tinnitus, or neurological symptoms are present.
Do not skip this process. A proper diagnosis is the foundation of effective management.
What Connects Almost All Causes
Despite the enormous variety of causes, almost all of them share a common final pathway: they alter the signals reaching the brain’s auditory cortex, and the auditory cortex responds by generating phantom sounds. This is why researchers increasingly describe tinnitus as a brain condition that is triggered by ear or body events — rather than an ear condition in the traditional sense. It also explains why approaches that support the brain’s auditory neural networks — alongside addressing the specific underlying cause — tend to produce the best outcomes. The ear may be where the problem starts. But the brain is where the sound is made. Understanding that distinction is the beginning of a more effective approach to tinnitus management — wherever on the spectrum your particular case falls.
Conclusion
What causes tinnitus? The honest answer is that the list is long —age-related hearing loss, noise damage, earwax, infections, medications, high blood pressure, head injuries, TMJ disorders, Ménière’s disease, stress, and more. But almost all of these causes share the same final mechanism: they alter the auditory signals reaching the brain, and the brain generates phantom sounds in response. If you have tinnitus and do not yet have a clear understanding of what is causing it — getting that answer is the most important step you can take. Not because knowing the cause makes the ringing stop immediately, but because it determines which management approaches actually apply to your situation. See your doctor. Ask for a proper audiological assessment. Pursue a diagnosis rather than a guess. And in the meantime — know that you are far from alone, that effective management is possible for most causes, and that understanding what you are dealing with is the most empowering thing you can do.
